Irritant and allergic reactions to essential oils
Fortunately, most people that use essential oils never experience any type of adverse reaction. However, some do, and in most cases their experience is both unpleasant and avoidable. In a few instances, the reaction has serious consequences. As always, our aim is to show you how to minimize risk so that you can use essential oils safely, as well as effectively.
Skin reactions are the most common types of adverse reaction to essential oils, and they include:
- Irritation (Irritant contact dermatitis)
- Allergic contact dermatitis (delayed hypersensitivity)
- Contact urticaria (immediate hypersensitivity)
Both contact urticaria and allergic contact dermatitis are allergic reactions, which are also known as hypersensitivities. (Photosensitization is not covered on this page.) If you are experiencing an adverse skin reaction, go here for guidelines on what to do.
What does an irritant or allergic reaction look like/feel like?
In most people, an irritant or allergic reaction starts to manifest within 5 or 10 minutes of applying an essential oil, and can be almost instant. Symptoms include some or all of the following:
- Redness

Adverse reaction to an extremely low dilution of
cinnamon bark and peppermint oils in a shampoo - Itching
- Burning and/or pain
- Hives (tiny blisters)
The initial symptoms are pretty much the same for both irritation and allergy, but while irritation reactions tend to resolve within a few hours, allergic reactions may persist for days or even weeks. Sometimes allergic reactions spread to parts of the body the oil was not directly applied to. Another difference is that greater dilution of an essential oil will usually prevent irritation from happening again, but this may not prevent subsequent allergic reactions.
Irritation
The medical term for the skin reaction to an irritant is “irritant contact dermatitis”. This is the least problematic type of skin reaction, and the inflammation dies down quite quickly after the oil is removed from the skin, though it is still unpleasant and undesirable. Common causes of irritation from essential oils include:
-
- Using undiluted or insufficiently diluted essential oils on the skin.
- Adding undiluted or poorly diluted essential oils to a bath
Click here for a case of irritation caused by Oregano oil.
{kind=link}
Several case reports can be found here.
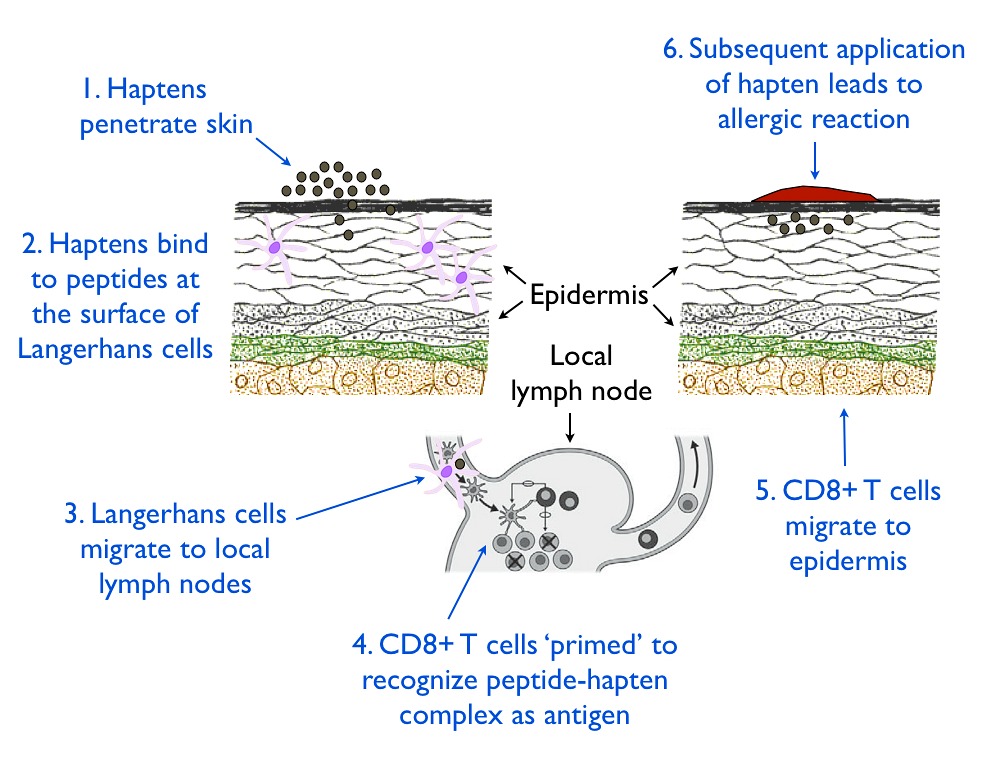
Allergic contact dermatitis
This is the most common type of adverse skin reaction to essential oils. It is also called delayed hypersensitivity because it does not occur the first time the skin is exposed to the substance. In a recent report, 3.9% of 4,238 dermatitis patients who were patch tested with cinnamaldehyde had a positive (i.e. allergic) reaction (Warshaw et al 2015). The mechanism that takes place involves the immune system, and is illustrated here:
There are complex reasons why this happens to some people and not others:
- Some essential oils, such as Cinnamon bark, Ylang-Ylang and Lemongrass, are more prone to causing allergic reactions than others. In most cases a single constituent (such as cinnamaldehyde in Cinnamon bark and citral in Lemongrass) is responsible.
- Dilution and risk are directly related. The more dilute an essential oil is, the lower the risk, and the more concentrated an essential oil is, the greater the risk.
- Women are at greater risk of allergic reaction to essential oils than are men. The reasons are probably hormonal.
- Frequency (how often an oil is applied per day) and duration (the number of days, weeks, months it is applied) are also factors, basically increasing risk.
- People who have, or who have had atopic dermatitis are at greater risk.
It’s interesting that there is often a correlation between people with seasonal allergies and those prone to skin allergies to essential oils. The reason for this link may be genetic, and/or may be due to immune-reacting cells migrating from one part of the body to another
An allergic reaction often will not happen the first time an essential oil is used.

Allergic reaction to a mix of undiluted Helichrysum, Lavender and Tea Tree oils
Contact urticaria and anaphylaxis
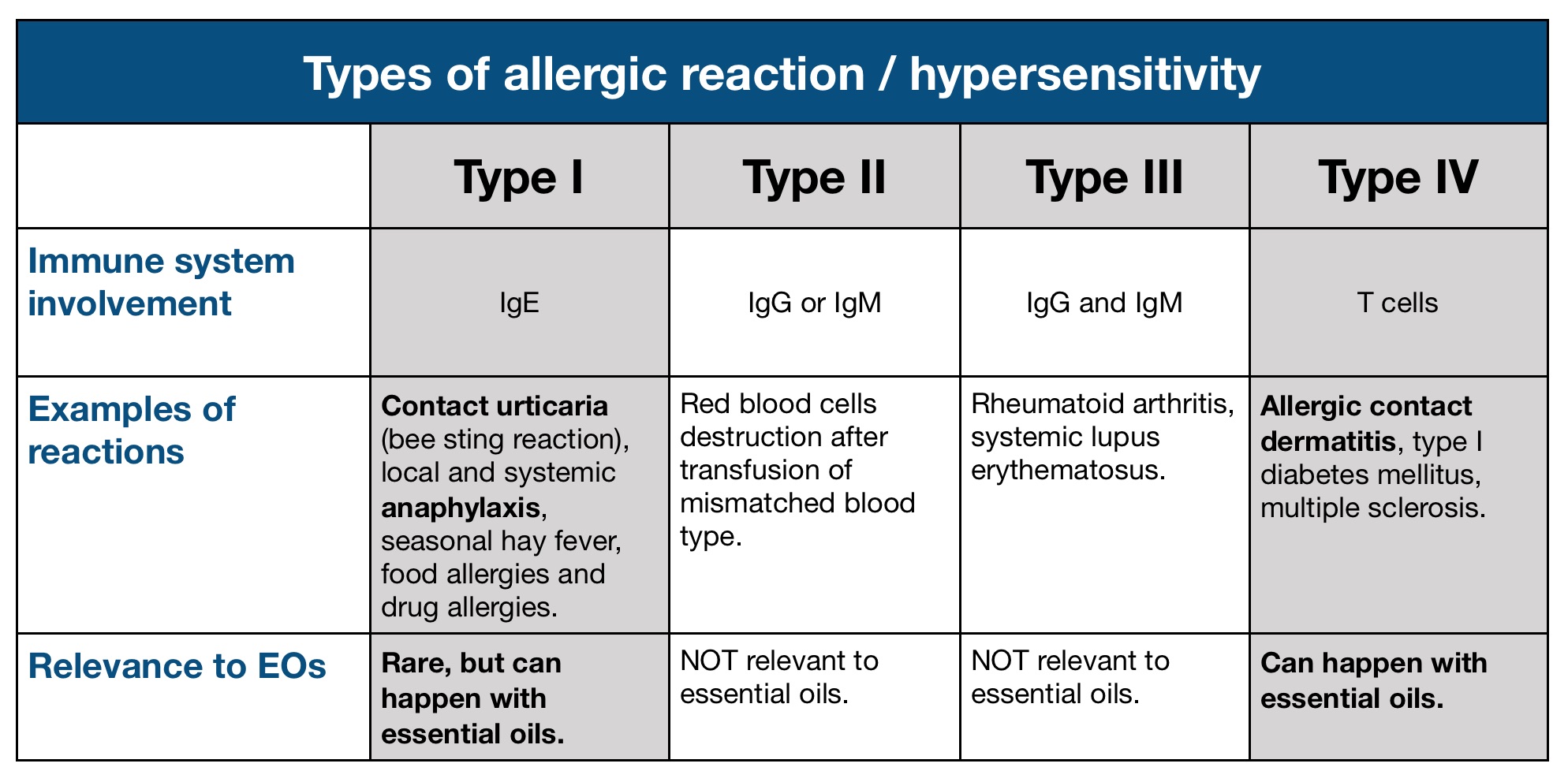
Contact urticaria is the same type of allergic reaction that some people get from a bee sting, and it causes a characteristic “wheal and flare” response (see illustration). Contact urticaria can either be immunological (IgE-mediated) (immunological contact urticaria, or ICU), or non-immunological (NICU). ICU can involve the respiratory system or the gastro-intestinal tract, and it can cause anaphylactic shock, which in turn may be fatal (Bhatia et al 2009, Davari & Maibach 2010).
{kind=link}

Example of contact urticaria
The following are all possible signs of anaphylaxis:
– Difficulty breathing
– Swollen lips, tongue, throat
– Blood pressure drops alarmingly
– Hives, redness, itching, which may be widespread
One case of probable anaphylaxis to cinnamaldehyde has been reported (Diba & Statham 2003), and there are two known cases, and two probable cases of anaphylaxis to essential oils in our Adverse Reactions Database. None of these were fatal, and these types of reaction are extremely rare with essential oils. You can view the details here, here, here and here.
Multiple hypersensitivities
In some cases, being allergic to an essential oil leads to multiple hypersensitivities – the person develops allergies to many essential oils, not necessarily because of common chemistry. In these types of cases, complete avoidance of all essential oils is recommended for several weeks. After this period, essential oils should only be reintroduced one at a time.
Tipping the scales
In a few cases, sudden and widespread allergic reactions develop following a long period of very intensive use of essential oils, both topically and orally. This can be simply described as the body saying enough is enough. Three examples of such reaction can be found here, here and here.
FAQ
Here are some frequently asked questions about essential oils and skin safety:
- What should I do if I experience and adverse skin reaction?
Please see this page: https://tisserandinstitute.org/safety/what-to-do-when-experiencing-an-adverse-reaction/
- How can I minimize the risk of irritation or allergic reaction?
- Do not use undiluted essential oils on the skin.
- Be careful when using essential oils in the bath
- Follow age-related safety guidelines
- Follow safety guidelines for high-risk essential oils (see Tables below).
- Avoid using the same oil or blend at more than 5% dilution for long periods of time (months/years).
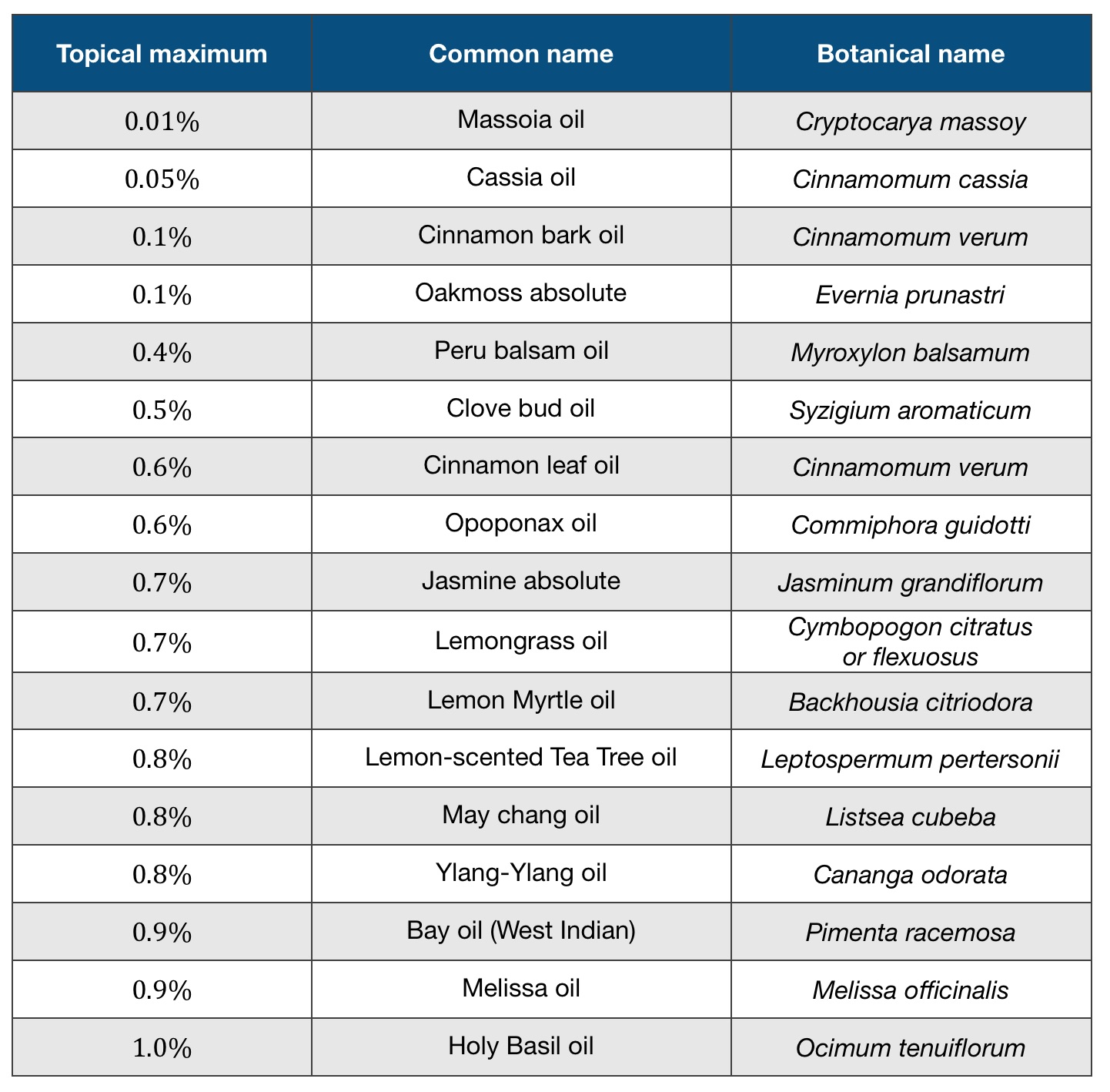
Here are dilution maximums for topical application of the most common essential oils and absolutes that carry the highest risk – their dermal maximum is 1.5% or less. Most of these are widely-recognized industry standards for pure essential oils, and they are guidelines for avoiding adverse skin reactions. Some people will be able to use more concentrated oils, but this is not advisable as it does increase risk. For more details consult Essential Oil Safety, 2e.
Irritant essential oils and their topical maximums:
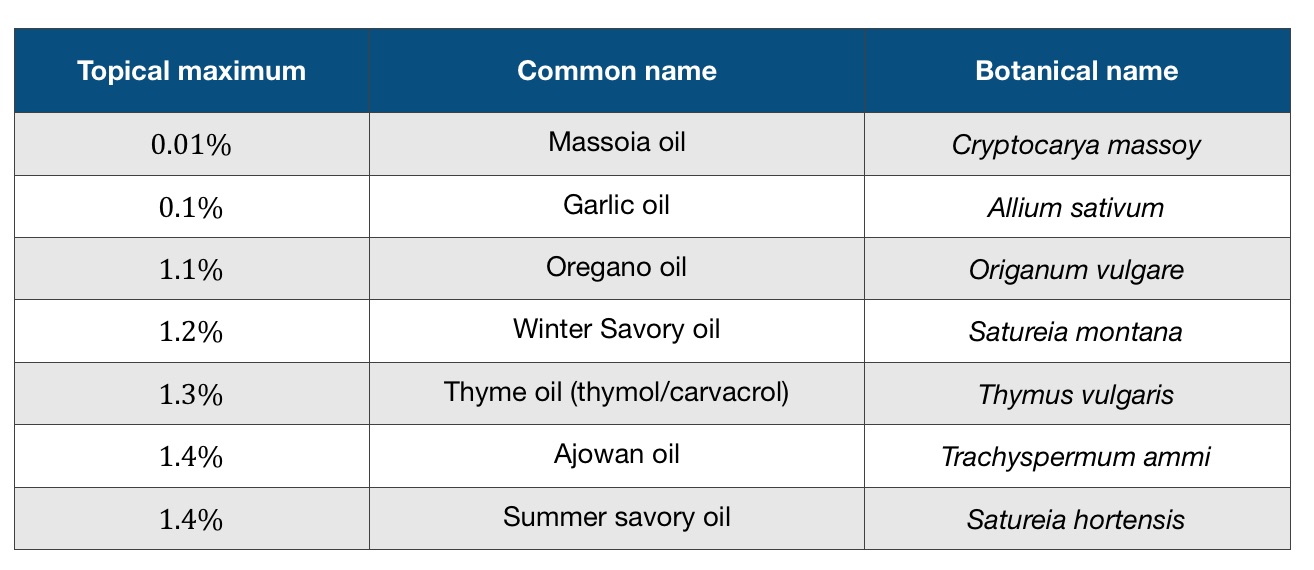
Allergenic essential oils and their topical maximums:
- What is “sensitization”?
The word “sensitization” is often misunderstood. It’s sometimes used as if it was a distinct category of adverse reaction – it isn’t – and it’s sometimes used as a synonym for an allergic skin reaction. This second use of the word does make sense, but really “sensitization” describes the priming of the immune system that subsequently leads to an allergic reaction. So it’s part of the process.
- What is a “hot oil”?
Technically speaking, there is no such thing. There are essential oils likely to cause irritation, and others that are likely to cause allergic reactions. There’s no reason why you can’t group them all together and call them “hot oils”, so long as you understand that each one has it’s own maximum dilution safety guideline. For the record, neither Black Pepper essential oil nor Ginger essential oil is a “hot oil”, so we think it’s a misleading concept.
- How long will my allergy last?
The acute phase of an allergic reaction usually lasts for several hours, and then the skin calms down. In a minority of cases, the reaction persists for weeks, and the use of steroids may be helpful. It’s important to note that if you re-apply the same essential oil or blend you may have another allergic reaction. This is because, once your immune system has been primed through T cells to recognize a constituent as an allergen, this generally persists for the rest of your life. In some people, allergies do resolve after 10 or 20 years, but not in everyone.
- If my skin becomes inflamed after applying an essential oil, is this a sign that I am detoxing?
No, it never is a sign that you are detoxing. Read more here.
- I have heard that you can’t have a true allergic reaction to an essential oil. Is this true?
You may hear that the constituents of essential oils are too small to be recognized by the immune system, or that we only mount allergic reactions to proteins, and essential oils don’t contain proteins. The last part is true – essential oils don’t contain proteins. However, essential oil constituents often chemically bind to proteins in the skin (this forms something called a “hapten-peptide complex”) and this combination molecule can be recognized by the immune system, leading to an allergic reaction (Chipinda et al 2011).
You may also hear that reactions to essential oils are “not true allergic reactions”. Most essential oil allergies are not IgE-mediated reactions like food allergies; this is the only type of allergic reaction that involves antibodies, and is known as Type 1 hypersensitivity. However, there are four classes of allergic reaction, and Type IV, delayed hypersensitivity, occurs through T-cell priming of the immune system.
So yes, it is possible to have an allergic reaction to an essential oil.
- Is an allergic reaction a sign that by body is not healthy?
The transdermal absorption of essential oil constituents happens more readily in people with disturbed skin “barrier function” (De Benedetto et al 2012, Egawa & Kabashima 2017). Some of these constituents may be potential allergens. The same barrier principle, and similar mechanisms, apply to food allergies and “leaky gut” (Mu et al 2017) and to inhaled allergies like allergic rhinitis and asthma and the lungs (Schleimer & Berdnikovs 2017). So disturbed barrier function in various tissues tends to make us more allergy-prone.
The skin’s barrier function is its ability to keep unwanted substances from being absorbed into the body, and if it is not functioning optimally, this increases the risk of both skin contact irritation and allergy. Various factors can affect barrier function such as stress, dry weather, and the skin’s microbiome (Prescott et al 2017). This does not take away from the reality of an allergic reaction, nor does it mean that it’s “your fault”. Here are some guidelines for improving and maintaining your skin’s barrier function.
- Is patch testing a good idea?
It depends, but in general we don’t recommend it. First, just to be clear, this is not a skin prick or scratch test (these test for IgE reactions, but most reactions to essential oils are not IgE-related). Second, patch testing can be useful, but there are drawbacks. It is normally carried out by a dermatologist, using specially prepared patches – which you can’t buy – and doing the test properly is laborious. Also, patch testing is not 100% reliable – sometimes there are false positives or false negatives. Finally, intensive patch testing itself occasionally produces allergic reactions that would not otherwise have occurred.
If you are planning to use essential oils on a high-risk individual, whether yourself or someone else, then we would recommend dose escalation (see below) instead of patch testing. A high-risk individual would be someone, for example, who has had one or more topical allergic reactions in the past, or someone who has multiple chemical sensitivity.
Dose escalation: Start with a low dilution – perhaps 1% – and then gradually increasing the concentration in 0.5% steps if there seems to be little effect initially.
References
Bhatia, R., Alikhan, A., & Maibach, H. I. (2009). Contact urticaria: present scenario. Indian Journal of Dermatology, 54(3), 264–268.
Chipinda, I., Hettick, J. M., & Siegel, P. D. (2011). Haptenation: chemical reactivity and protein binding. Journal of Allergy, 2011, 1–11.
Davari, P., & Maibach, H.I. (2010). Contact urticaria to cosmetic and industrial dyes. Clinical & Experimental Dermatology, 36, 1-5.
De Benedetto, A., Kubo, A., & Beck, L. A. (2012). Skin barrier disruption: a requirement for allergen sensitization? Journal of Investigative Dermatology, 132(3), 949–963.
Diba, V. C., & Statham, B. N. (2003). Contact urticaria from cinnamal leading to anaphylaxis. Contact Dermatitis, 48(2), 119.
Egawa, G., & Kabashima, K. (2017). Barrier dysfunction in the skin allergy. Allergology International, 67(1), 3–11.
Mu, Q., Kirby, J., Reilly, C. M., & Luo, X. M. (2017). Leaky gut as a danger signal for autoimmune diseases. Frontiers in Immunology, 8(May), 1–10.
Prescott, S. L., Larcombe, D. L., Logan, A. C. et al (2017). The skin microbiome: Impact of modern environments on skin ecology, barrier integrity, and systemic immune programming. World Allergy Organization Journal, 10(1), 1–16.
Schleimer, R. P., & Berdnikovs, S. (2017). Etiology of epithelial barrier dysfunction in patients with type 2 inflammatory diseases. Journal of Allergy and Clinical Immunology, 139(6), 1752–1761.
Warshaw, E. M., Maibach, H. I., Taylor, J. S et al (2015). North American Contact Dermatitis Group patch test results: 2011-2012. Dermatitis: 26(1), 49–59.