
Lemongrass decoction being prepared: Pucallpa, Peru. © Kelly Ablard
This study was the first of its kind carried out in Peru to identify and understand the use of aromatic plant medicine (APM) as a form of traditional medicine from the viewpoint of Aromatherapy as practiced in North America, and to assess the conservation status of Peruvian aromatic medicinal plants. Informants (plant-medicine healers and locals) were surveyed and interviewed. Results revealed that APM is highly respected throughout Peru, and critical to its traditional medicine system. Sixty-three aromatic medicinal plants were identified, along with the conditions they are used to treat, and common extraction and application methods. Factors impacting the abundance of aromatic medicinal plants and their conservation statuses were also revealed. The majority of informants who use APM do so sustainably; they were aware and concerned that their medicine is disappearing as a result of deforestation, overharvesting, and climate change. Reforestation is one strategy being implemented to help conserve their valued plants. Collaborative efforts are now underway to help preserve and strengthen the Peruvian knowledge base of aromatic plants and their use in traditional medicine, and also to increase global awareness of endangered essential oil–bearing plants.
Introduction
Peru is a South American country that includes 13% of the Amazon jungle where an extraordinary amount of biodiversity exists (Marchese, 2015). The total number of plant species, including aromatic plants with known medicinal properties, rates fifth in the world (Bussmann, 2013). Medicinal plants contribute ~ $1.2 million US annually to the Peruvian economy (Bussmann et al., 2007), and traditional medicine (TM), also referred to as complementary/alternative medicine (CAM), has a strong presence in Peruvian culture (Monigatti et al., 2013; WHO, 2013).

Maceration of medicinal plants: Pucallpa, Peru. © Kelly Ablard
The use of TM in Peru was recorded in the 15th century, when Inca healers used plant medicine along with religion and magic to treat many diseases (Elferink, 2015). These healing practices, which included ceremonies, rituals, and sacred places, are still prevalent in the daily life of Peruvian communities today (Jauregui et al., 2011). For example, there are reports that traditional modern-day healers use incense, flower petals and the extraction of all plant parts as medicine in their healing practice, ceremonies, and rituals to help combat disease, relieve anxiety, enhance mental well-being, and protect against negative spirits (Gonzales de la Cruz et al., 2014). This example parallels the essence of Aromatherapy, a CAM defined in North America as “the art and science of utilizing naturally extracted aromatic essences from plants to balance, harmonize and promote the health of body, mind and spirit. It seeks to unify physiological, psychological and spiritual processes to enhance an individual’s innate healing process” (NAHA, 2016). Whether Aromatherapy is practiced in Peru remains uncertain, but given the above example and evidence that 15% of CAM in central Peru is “floral therapy” (i.e. the use of aromatic essences for healing) (Lovera and Fuentes, 2013), there is a strong likelihood that Aromatherapy, or a form thereof, is being implemented. Also supporting the use of aromatic plant medicine (APM) in Peru is the fact that the healing process for 50% of the Latin American population in both rural and urban settings begins and ends with TM as it is the only accessible and affordable medicine available (Albán, 1984; Bussmann et al., 2011; Jauregui et al., 2011; Bussmann, 2013). And it is often the preferred treatment; even those who can obtain allopathic medicine generally opt to protect and conserve their indigenous medical systems with their traditional knowledge of, and healing practices using traditional plant medicine (Jauregui et al., 2011).

Dr. Juan Ruiz shaving bark off an aromatic medicinal tree: Amazon Jungle, Peru. © Kelly Ablard
Traditional medicine/CAM not only costs less than allopathic medicine, but it often works better and certainly has fewer side effects. As a result, TM/CAM practice has gained the respect of government agencies and health providers in Peru, as well as those in developed countries (Bussmann, 2013; Caceres Guido et al., 2015). Consequently, the demand for medicinal herbs has increased. This high demand, coupled with deforestation, climate change, urban sprawl, mining activities, and pollution, has negatively impacted the sustainability of many medicinal plants – ones that Peruvian communities heavily rely on (Bussmann et al., 2007; Caceres Guido et al., 2015; IUCN, 2016). Unfortunately, there is a severe gap in our knowledge base of how these factors have negatively impacted aromatic medicinal plants. Therefore, the objectives of this study were to: 1) Identify the Peruvian aromatic plants being used as medicine 2) Gain an understanding of the knowledge and practice of APM in Peru, especially in relation to Aromatherapy, as practiced in N. America 3) Identify factors impacting aromatic plants and their conservation status 4) Explore the sustainability and conservation efforts already in place to protect aromatic medicinal plants.
Methods and analysis
Qualitative data and plant specimens were collected during the month of October, 2015. Data collection occurred in northern (Iquitos and Amazon jungle), central (Lima and Pucallpa), and southern (Cusco and Pisac) Peru. Informants were selected based on purposive (i.e. sampling pre-selected informants), snowball (i.e. sampling informants obtained through referrals), and convenient sampling (i.e. sampling informants not pre-selected or referred, but close in proximity) (Bernard, 2006). All participants were verbally informed about the objectives of the study and were free to withdraw at any time. Prior to surveying and interviewing, informed consent was obtained from each individual and from their community when necessary (Monigatti et al., 2013). Structured surveys and semi-structured interviews focused on the interviewees’ understanding, attitudes, and practices relating to modern medicine and traditional APM (Williamson et al., 2015).

Aromatic medicinal plants: Belen Market, Iquitos, Peru. © Kelly Ablard
All surveys (n=10) and interviews (n=23) were completed with the author present, with one exception. Survey questions were written in both English and Latin American (LA) Spanish; interview questions were spoken in English. When necessary, questions were translated to LA Spanish or Quechua with the help of a native Spanish- and Quechua-speaking translator. In some cases, answers in the form of written text were not possible, so survey questions were read out loud to interviewees, and audio or video recordings were made. Informant answers were translated into English when necessary. Recordings were also taken during healing ceremonies and of native pakos, curanderos, ibos, ayahuasceros, and shamans (denoted as healers) or locals (collectively denoted as informants) while they were purchasing, harvesting, or sharing knowledge about aromatic medicinal plants (Gonzales de la Cruz et al., 2014). Plant conservation statuses were derived from IUCN Red List (2016) using the following search criteria: taxa – species, subspecies and varieties; taxonomy – plantae (native, introduced, vagrant, and uncertain); location – Peru; systems – terrestrial. Data were entered into Microsoft Excel v.14.0. whereby descriptive statistics were generated.
Peruvian aromatic medicinal plants
Sixty-three aromatic plants were identified, all of which are used in healing practices to prevent or treat disease. Conditions included psychosomatic disorders, anxiety, nervousness, depression, respiratory disorders, headache, arthritis, rheumatism, inflammation, insect bites, infection, cold, flu, sepsis, stomach ache, fatigue, bad wind,1 limpia,2 susto,3 and magic (Table 1). Plants belonging to the Lamiaceae family were recorded most frequently followed by plants in the Lauraceae family (Table 1). Plants within these two families are known to contain essential oils with anti-inflammatory, anti-microbial, and anti-mutagenic properties (Raut and Karuppayil, 2014). Plants belonging to the Myrtaceae and Rutaceae were also recorded. Plants in these families have substantial ethnobotanical, pharmacological and economic value because of their medicinal essential oils (Table 1) (Raut and Karuppayil, 2014).

Table 1. Botanical and conservation statuses of Peruvian aromatic medicinal plants and their use in traditional medicine (click to download in full)
Different aromatic medicinal plants were identified in each study area within northern, central, and southern regions, and on occasion, the same plant was found to be utilized throughout all regions (Table 1). Depending on location, healers and locals obtained aromatic plants either solely from the wild, markets, and/or home gardens. Plants found in the market were typically fresh and whole even though the whole plant was not always used in medicine (Table 1). Aromatic medicinal plants, either infused for love potions (pusangas), or in powder form for use as dietary supplements, were also abundant in the markets. Steam-distilled essential oils were found for purchase in one market and on the street.

Essential oils steam-distilled in Cusco, Peru. © Kelly Ablard
1Bad wind or wayra symptoms include vomiting, headache, stomach ache, sore feet, paleness, fatigue, cold body, paralysis, and the inability to speak caused by animal or spiritual encounters at night (Mathez-Stiefel et al., 2012). 2 Limpia is a cleansing ceremony. 3 Susto is sadness for long periods, crying without reason, feeling empty, and insomnia caused by evil energy (Monigatti et al., 2013).
The practice of aromatherapy in Peru
Aromatherapy, as defined above, is a form of TM used often as a first-line treatment throughout Peru. Aromatic plant medicine was considered crucial to healing by 100% of the informants questioned; according to an Andean healer “the aromatic essence of the plant is very powerful.” These “powerful essences” were utilized by both males and females who ranged in age from 4 to 74 (Figure 5) and varied in both healer and non-healer professions. A Shipibo teacher said he uses APM because it is “all healing, mind-balancing, and a source of strength.”

Shipibo family preparing aromatic bath containing aromatic medicinal plants: Pucallpa, Peru. © Kelly Ablard
Unlike certified and registered Aromatherapists, users of APM in Peru do not obtain their knowledge through formal education. Eighty-seven percent of the informants gained their knowledge through oral records and plantas con madre (plants that teach). These, according to Bussmann et al. (2007), are the most common sources of knowledge about plant medicine in Peru. It’s important to appreciate that, although there is a strong knowledge base in place, healers are always trying new remedies and want to learn more about plant medicine (Jauregui et al., 2011). This corroborates this study’s findings whereby 90% of the healers expressed their desire to learn more about essential oils. For example, when an Amazonian healer was introduced to an essential oil for the first time, he spent hours examining it, questioning its therapeutic properties and applications, and connecting with the plant’s spirit. Dr. Rojas, a university professor in Peru who studies essential oils, told me that knowledge should be strengthened through implementation of more structured education and scientific research in the field of Aromatherapy. This would satisfy the curiosity of, and credibility behind, aromatic medicinal plant healers. Each informant knew something about naturally producing aromatic extracts from fresh plant material, and which methods produced less toxins (Bussmann et al., 2011). Extractions were done on the whole plant, leaves, resin, stems, roots, bark, wood, and flowers (Table 1). Extraction methods included alcohol extraction (tincture), water extraction (infusion or decoction), heat extraction, lipid extraction (infusion), maceration (i.e. crushing) and steam distillation. Water extractions and maceration were the two extraction methods I most frequently observed, solvent and heat extraction methods were the most frequently spoken about, and steam distillation was the least used and understood method.

Homemade steam distiller: Pucallpa, Peru. © Kelly Ablard
Solvent extractions of aromatic medicinal plant oils were done with sugar cane alcohol; this is a well-documented solvent used throughout Peru (Bussmann et al., 2011). Either cold or boiling water was used for water extractions, and fire was used for heat extractions. For example, a Cocama healer explained that leaves and bark are placed onto a fire to release chemicals and resins. The animal fat of snake, mule, chicken, or guinea pig is commonly used for lipid extractions (Bussmann and Glenn, 2011), but I did not see this method used. Plant material was macerated (crushed) with a mortar and pestle, knives, wooden spoons, but mostly with bare hands (Video 1). Steam distillation techniques and equipment varied as this method is the most expensive to employ (Video 2). Applications of APM were the same as those in North America – inhalation, topical, and oral. Applications were used solely and in combinations. Inhalation and topical applications occurred most frequently (Table 1). Inhalation of steamed plant material, Tobacco (Nicotiana rustica) smoke, bottled essential oils, smoke from burning wood, and synthetic perfumes (e.g. Tabu and Florida water) was also very common in ceremonies, rituals, and healing practices. The inhalation of steam from boiled leaves of Muña (Minthostachys mollis) was used to clear congestion, the smoke from Tobacco was blown over a person by a healer while using ikaros 4 to purify the air and the person, the essential oil of Palo Santo (Bursera graveolens) was inhaled to relax the mind, and smoke from woods such as Palo Santo and Canela Sacha (Cinnamomum verum) were used as incense with smoke inhaled for treatment of evil wind or colds. Nasal ingestion of Tobacco juice is also commonly done to ward off evil spirits (Bussmann, 2013), but I did not see this.

Love potions (pusangas): Belen market, Iquitos, Peru. © Kelly Ablard
4 Ikaros are songs or whistles of sacred melodies (Jauregui et al., 2011). Visit www.kellyablard.com for an audio sample of an ikaros. Topical applications included compresses, poultices, and essential oils blended with Jojoba (Simmondsia chinensis) oil, Copaiba (Copaifera sp.) oil, or Coconut (Cocos nucifera) oil to be sprayed onto the whole body or applied to a specific body part. For example, an Andean healer’s treatment for muscle pain was to combine crushed Molle (Schinus molle) and Eucalyptus (Eucalyptus globulus) leaves in a bowl of sugar cane alcohol for 7–15 days; the liquid was then used as a compress for sore muscles. Crushed plant material to help clear negative energy was placed onto the skin between the upper and lower arm, and Andean Bog Myrtle (Myrteola nummularia) essential oil was combined with a carrier oil for application to the face to reduce wrinkles.
Shipibo family preparing aromatic bath containing aromatic medicinal plants: Pucallpa, Peru. © Kelly Ablard
The combination of inhalation and topical applications came in the form of flower baths a.k.a. aromatic baths or baños de florecimiento (flourishing or invigorating baths). These were either bathtubs or small buckets filled with water and 5–9 aromatic medicinal plants. Aromatic baths were extremely common and were used in daily practice to enhance rituals and heal a number of specific conditions. Mostly they were used to clear the mind, give strength, combat disease caused by evil spirits, treat psychosomatic disorders, fend off evil spirits, or to attract and send love (Table 1) (Figure 9). Baths were taken over the course of 3 days (1 bath per day) and were thought to only be effective if you repeatedly inhaled the aroma of the plants and poured them over your head. Oral applications included ingestion of infusions, or of essential oils. One drop of Palo Santo essential oil mixed with warm water and ingested daily was used to strengthen immunity. Two drops of Muña essential oil mixed with warm water were ingested twice a day to relieve symptoms associated with bronchitis, asthma, and colds. Ingestion of a Lemongrass (Cymbopogon citratus) decoction would aid digestion. Note that some of these species may in fact be endangered in other countries due to being overharvested for medicinal use. Unless noted otherwise, this table provides data only obtained within the confines of this study. 1 Jernigan (2012), 2 Bussmann et al., 2010, 3 Monigatti et al., 2013, 4 Sanz-Biset et al., 2009
Factors impacting Peruvian aromatic plants and their conservation status
There is a heightened awareness among Peruvians of the impact of deforestation and overharvesting on the stability of aromatic medicinal plants. Eighty percent of the informants stated it is increasingly difficult to find aromatic medicinal plants in their natural state, and 100% were concerned about the problem worsening. Overharvesting and climate change were spoken of often. One healer said, “There are hundreds of plants I can no longer find, because everyone uses them.” For example, Rosewood (Aniba rosodora) is harvested for the production of the essential oil obtained from the wood. According to the IUCN (2016), when Rosewood is harvested, the whole tree, along with its root system, is destroyed. Additionally, both mature and immature trees are being harvested, and signs of regeneration are absent. Therefore, little is being preserved for future generations and unless something drastically changes, Aniba rosodora will disappear.

Tree seedlings to be planted in communities as part of a reforestation project: Pucallpa, Peru. © Kelly Ablard
Climate change is another serious issue. For example, due to a shortage of water, one Andean healer stated his community finds it difficult to source aromatic medicinal plants because animals are quickly eating them to stay hydrated (Victor, personal communication, Oct. 23rd, 2015). And in the Amazon jungle, there has been an increase in flooding which has impacted the growth of, and accessibility to, medicinal plants (Jairo, personal communication, Oct. 13th, 2015). The conservation status of Peruvian plants on the IUCN Red List (2016) (n = 751) may very well include a number of the plants informants spoke of which may not have been aromatic and/or were not identified. The aromatic medicinal plants identified varied in conservation status from unknown to critically endangered (Table 1). However, a plant with unknown status or no status may in fact have a status of concern. More survey data on the status of these plants needs to be collected.
Sustainability and conservation efforts of Peruvian aromatic medicinal plants
Informants shared some strategies they use locally to address the aforementioned problems. One community has built a greenhouse which serves a dual function: one, it gives them more control over the environment that their aromatic medicinal plants are grown in, and two, the plants are protected from animals that eat them as a source of hydration. Some informants have committed to only using aromatic medicinal plants grown in home gardens instead of harvesting them from the wild, and more than half the informants that harvest plant material from the wild are replanting what they take. For example, in southern Peru, a reforestation project has been established whereby medicinal plant seeds are banked and wild-harvested plants are replanted in their natural habitat (Figure 11). There are also reforestation projects targeting Rosewood (A. rosodora), but their viability is unclear. Harvesting and/or distilling Rosewood requires a CITES permit as a result of it being classified as endangered. However, I attempted to communicate with two distillers in Peru who apparently meet these standards, and neither would answer questions relating to their practice, nor allow persons on their property. World-recognized expert on medicinal plants and curator of the Herbario Amazonense, Dr. Juan Ruiz (Figure 12) strives to strike a balance between sustainable practices and conservation of aromatic medicinal plants. There are a number of aromatic medicinal plants that he knows are abundant, and are not in imminent danger of critical conservation status (Table 2). It is his hope to preserve this relationship and help with reforestation projects geared toward APM.
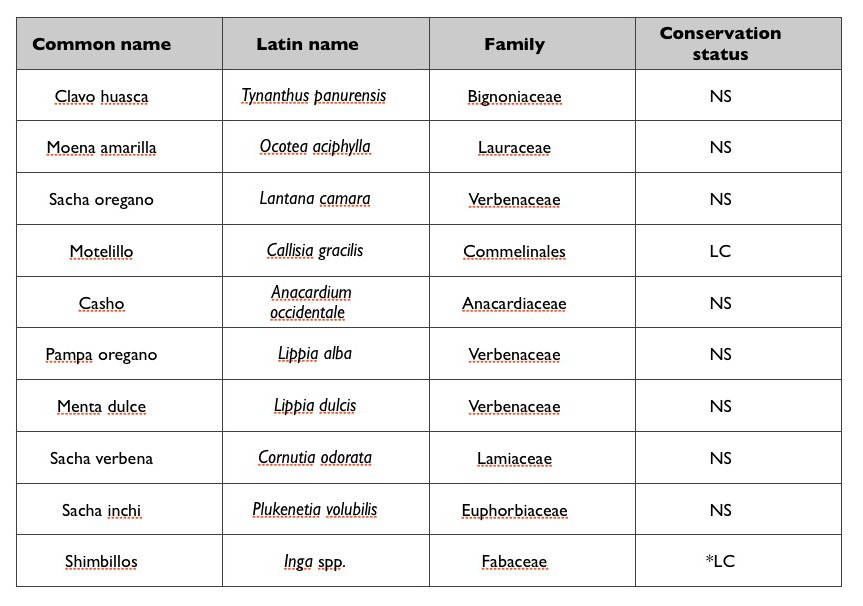
Table 2. Abundant Peruvian aromatic medicial plants. Note that casho is cashew.
NS = No Status; LC = Least Concern. *A small percentage of Inga spp. are vulnerable.
Conclusion and future direction
This was the first study carried out to explore the identification and use of traditional APM in Peru. There is compelling evidence that Peruvians practice a form of Aromatherapy, which is “the art and science of utilizing naturally extracted aromatic essences from plants to balance, harmonize and promote the health of body, mind and spirit….” (NAHA, 2016). Although Peruvians are using “Aromatherapy” in their daily lives, they still aim to learn more about APM and its uses. Consequently, efforts are underway to provide educational instruction on the chemistry and therapeutic values of essential oils, as well as cost-effective ways of extraction with higher yields of essential oil. The latter is critical considering that their aromatic medicinal plants are fewer in number and even disappearing, because of climate change, overharvesting, and deforestation.

Macerated aromatic plants placed on arm
to clear negative energy: Iquitos, Peru.
© Kelly Ablard
Peruvians have taken steps to help conserve and protect their APM for its use in local healing by future generations, but doing so can be costly and require resources difficult to obtain. We can help by: 1) sharing their wisdom of APM which helps to protect and conserve their traditional knowledge and practices which are critical to their preservation. 2) establishing sustainable methods of growth and harvesting of essential-oil bearing plants in Peru, and providing a market for the oils which will not only help conserve plants, but also help communities become economically independent. 3) collaborating with Peruvian universities to help demonstrate scientifically the therapeutic value of their APM. 4) not purchasing products that contain essential oils that are sourced unsustainably. 5) not using essential oils sourced from endangered plants; for example, there are alternative essential oils with similar properties and therapeutic activity to Rosewood. And finally, in the words of Peruvian plant-medicine healer Javier, “let’s not forget that plants are the master healers and teachers which help us gain greater awareness of our planet and the universe as a whole – they remind us to come home to ourselves.”
Limitations
Although the structured surveys were limited in sample size, ethnobotanical data obtained by semi-structured interviews combined with a thorough review of germane literature, strengthens the observations drawn from these results and discussion. Additionally, some data were not introduced into the study due to translation difficulties and importation of plant samples into North America for identification. d
Acknowledgements
This research was possible thanks to Gary Ablard (padre), Gary Ablard II, Patris Aghakian, Jose Felix Arevalo, Robert Arndt, Crystal Baldwin, Jim Barry, Brian Beacham, Hana Viola Belikova, Hannah Bottomley, Judy Boyd, The Bozic Family, Kristin Clark, Peter Cramer, Jacqueline Dale, Nicole Degagne, Niko Dorje, Robert Dowdell, Diane Dunn, Flying Dog (Marcel), Jeffrey Boyd Garrison, Omar Gomez, Aaron Heriford, Julieta Herrera, Bernard Houston, Victor Hugo Yana Huaman, Jairo Ibreno, Zaid Jumean, Joan Keith, Janet Latter, Steve Laut, Iris Mori Lomas (Edie), Kate (Moss) Lila Rodriguez Lomas, Joel Lomas Maldonado, Obed Loma Maldonado, Panna Majithia, Dr. Charles Mango, Onour Moeri, Antonio Montero Pisco, Virginia Mori Sinuiri, Casey Mulcaster, Dr. Anna Nekaris, Linda Passmore (madre), Kirti Patel, Pedro, Walter Pena, Rene Picard, Satyen Raja, Javier Regueiro, Suzanne Rickards Raja, Star Riparetti, Dr. Rosario Rojas Duran, Dr. Juan Ruiz, Victor Serrubio, Geoff Smith, John Steele, Adam Stone, Colleen Thompson, Robert Tisserand, The Tisserand Institute, Universidad Nacional de la Amazonia Peruana, Universidad Peruana Cayetano Heredia, Lila Maldonado Urquia, Leah Ursic, Karla Vasquez, Veronika Vojtova, Graham Webber, Raoul ‘Wolf Man,’ Charlene Wood, and Nilo Zambrano.
Videos
Video 1: Maceration of leaves for aromatic bath performed by plant-medicine healer Antonio Montero Pisco. Iquitos, Peru. http://bit.ly/1QfSdF5 ©Kelly Ablard
Video 2: Steam distillation of Muña (Minthostachys mollis) in Cusco, Peru. http://bit.ly/1odorKu Permission granted by Instituto para la preservacion medicina inka.
References
Albán J. (1984). Plantas medicinales usadas en Lima para los trastornos digestivos. Thesis. Facultad de Ciencias Biologicas, Universidad Nacional Mayor de San Marcos, Lima, p190.
Bernard H R. (2006). Research Methods in Anthropology: Qualitative and Quantitative Approaches. 4th ed. Oxford, UK: AltaMira Press. p186–194.
Bussmann R W, Sharon D, Vandebroek I, Jones A, Revene Z. (2007). Health for sale: the medicinal plant markets in Trujillo and Chiclayo, Northern Peru. Journal of Ethnobiology and Ethnomedicine 3 (37), p1–9.
Bussmann R W, Glenn A, Sharon D. (2010). Antibacterial activity of medicinal plants of Northern Peru – can traditional applications provide leads for modern science? Indian Journal of Traditional Knowledge. 9 (4), p742–753.
Bussmann R W, Malca G, Glenn A, Sharon D, Nilsen B, Parris B, Dubose D, Ruiz D, Saleda J, Martinez M, Carillo L, Walker K, Kuhlman A, Townesmith A. (2011). Toxicity of medicinal plants used in traditional medicine in Northern Peru. Journal of Ethnopharmacology. 137, p121–140.
Bussmann R W and Glenn A. (2011). Fighting pain: Traditional Peruvian remedies for the treatment of Asthma, Rheumatism, Arthritis and sore bones. Indian Journal of Traditional Knowledge. 10 (3), p397–412.
Bussmann R W. (2013). The Globalization of Traditional Medicine in Northern Peru: From Shamanism to Molecules. Evidence-Based Complementary and Alternative Medicine. Available: doi:10.1155/2013/291903. Last accessed 20 January 2016.
Caceres Guido P, Ribas A, Gaioli M, Quattrone F, Macchi A. (2015). The state of the integrative medicine in Latin America: The long road to include complementary, natural, and traditional practices in formal health systems. European Journal of Integrative Medicine. 7, p5–12.
Elferink J G R. (2015). The Inca healer: empirical medical knowledge and magic in pre-Columbian Peru. Revista de Indias. LXXV (264), p323–350.
Gonzales de la Cruz M, Baldeón Malpartida S, Beltrán Santiago H, Jullian V, Bourdy G. (2014). Hot and cold: Medicinal plant uses in Quechua speaking communities in the high Andes (Callejón de Huaylas, Ancash, Perú). Journal of Ethnopharmacology. 155, p1093–1117. International Union for Conservation of Nature and Natural Resources (IUCN). (2016). The IUCN Red List of Threatened Species. Available: http://www.iucnredlist.org/. Last accessed 2 February 2016.
Jauregui X, Clavo Z M, Jovel E M, Pardo-de-Santayana M. (2011). “Plantas con madre”: Plants that teach and guide in the shamanic initiation process in the East-Central Peruvian Amazon. Journal of Ethnopharmacology. 134, p739–752.
Jernigan K. (2012). Plants with Histories: The Changing Ethnobotany of Iquito Speakers of the Peruvian Amazon. Economic Botany. 66 (1), p46–59.
Lovera, A and Fuentes, D. (2013). Identification of activities related to the practice and type of complementary and alternative medicine in Lima and Callao (Peru). Vitae-Revista de la Facultad de Quimica Farmaceutica. 20 (2), p118–124.
Marchese C. (2015). Biodiversity hotspots: A shortcut for a more complicated concept. Global Ecology and Conservation. 3, p297–309.
Mathez-Stiefel S-L, Vandebroek I, Rist S. (2012). Can Andean medicine coexist with biomedical healthcare? A comparison of two rural communities in Peru and Bolivia. Journal of Ethnobiology and Ethnomedicine. 8 (26), p1–16.
Monigatti M, Bussmann R W, Weckerle C S. (2013). Medicinal plant use in two Andean communities located at different altitudes in the Bolívar Province, Peru. Journal of Ethnopharmacology. 145, p450–464. National Association for Holistic Aromatherapy (NAHA). (2016). Available: www.naha.org. Last accessed 20 January 2016.
Raut J S and Karuppayil S M. (2014). A status review on the medicinal properties of essential oils. Industrial Crops and Products. 62, p250–264.
Sanz-Biset J, Campos-de-la-Cruz J, Epiquién-Rivera M A, Cañigueral S. (2009). A first survey on the medicinal plants of the Chazuta valley (Peruvian Amazon). Journal of Ethnopharmacology. 122, p333–362.
Williamson J, Ramirez R, Wingfield T. (2015). Health, Healthcare Access, and Use of Traditional Versus Modern Medicine in Remote Peruvian Amazon Communities: A Descriptive Study of Knowledge, Attitudes, and Practices. The American Society of Tropical Medicine and Hygiene. 92 (4), p857–864. World Health Organization. (2013). WHO Traditional Medicine Strategy 2014–2023. Geneva, Switzerland. Available: http://apps.who.int/iris/bitstream/10665/92455/1/9789241506090_eng.pdf?ua=1. Last accessed 31 January 2016.
0 Comments