
With thanks to Hana Tisserand for her input.
You probably know that most authorities advise dilution of essential oils before use, especially if applying to the skin. There are many reasons to dilute, and we will go through them here, along with an explanation for different dilution ranges. Products consisting of only essential oils have limited uses, and can be massively expensive, depending on content. Safety is another compelling reason for stretching out essential oils, whether because you want to avoid potential adverse effects, or to comply with safety regulations. We will explore this in detail below.
First, a few basic facts:
- When we talk about dilution or concentration, we are referring to the amount of one substance in a mixture. For example, if we talk about a 5% dilution, we mean that in the total product there is 5% of an essential oil and 95% of “other stuff”, and they cannot be easily separated.
- I will be talking in percentages, because they are universal. A percentage can be converted to any measurement – drops, milliliters, fluid ounces, grams etc.
- In calculating dilution, we can work with either weight or volume. What we can’t do is mix them up – you need to stick with one or the other.
- Conversion rates that use drops are always approximate, because no two drops of essential oil are the same.
- Sometimes you will see ratios, such as 1 part essential oil in 4 parts FCO (fractionated coconut oil).
- These ratios may be unsafe. For example, 1 in 4 means 25%, which is going to be much too concentrated for almost any safe use.
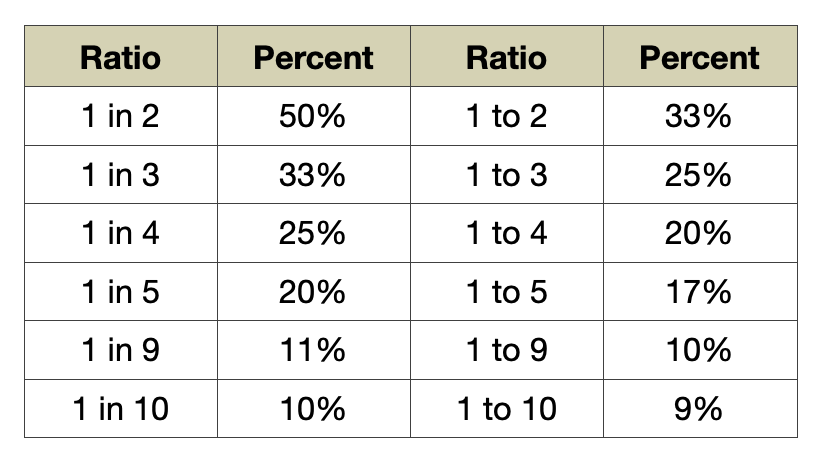
Ratios can be confusing, as the particle used (in or to) makes a significant difference! If you say 1 in 2, that means a one to one (50/50) ratio. On the other hand 1 to 2 ratio means one out of a total of three (33/67 ratio). The important consideration is always how many parts there are in total.
TRP channels
A major reason, if not the main one, to dilute essential oil is to avoid skin irritation or other skin reactions. We know essential oils can be anti-inflammatory and help in restoring our skin’s barrier function. We also know that the action of an essential oil on the skin is dilution-dependent – the greater the concentration of essential oil, the greater the risk of adverse reaction. Let’s look at why that is, and what are the mechanisms involved in both therapeutic and adverse effects.
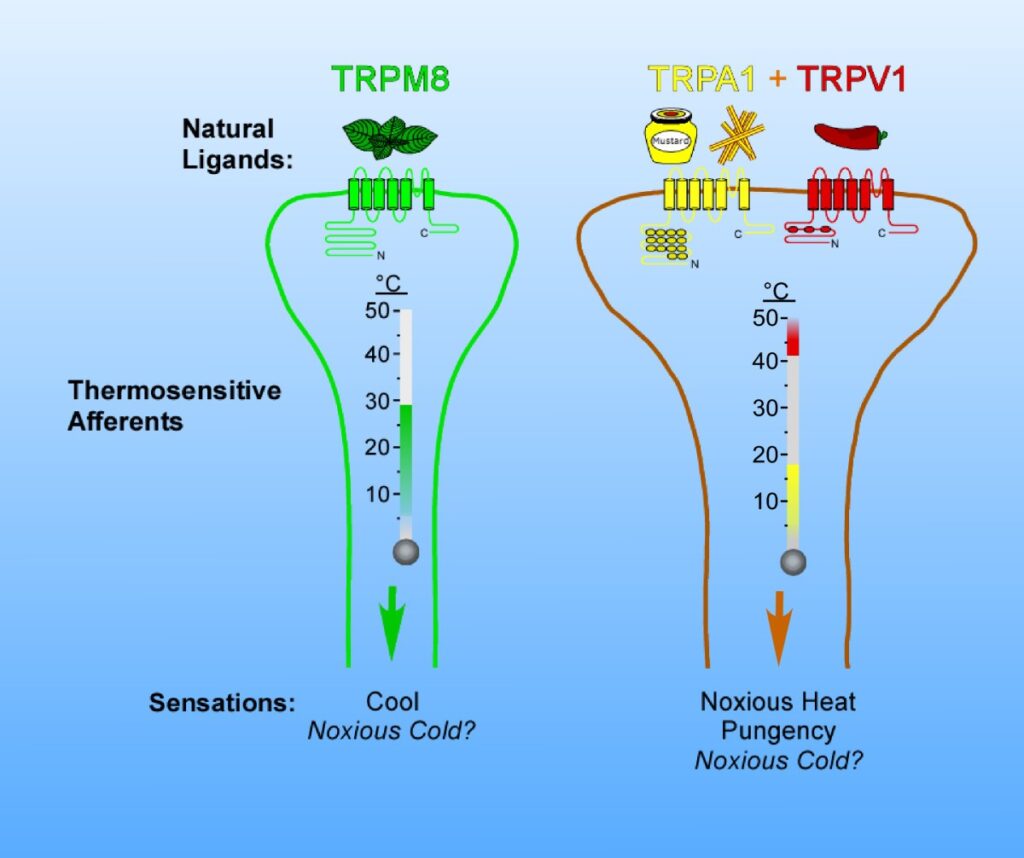
One of the functions of our skin is to warn us of danger through uncomfortable sensations such as irritation. The skin contains a class of receptors called transient receptor potential (TRP) channels that register sensations such as heat, cold, pain and irritation. They serve as an alert system to encourage us to change our behavior and avoid injury. If you ignore that signal and don’t move away from the source of heat etc., the body will send you a stronger signal in the form of – typically – pain. TRP channels are found not only on the surface of our skin, but in other epithelial tissue such as in our gut and airways.
An illustration of three TRP channels
Many essential oil constituents activate certain TRP channels. Some constituents are more activating than others, which is why oils such as Clove (eugenol), Cinnamon (cinnamaldehyde), Oregano (carvacrol) and Thyme (thymol) tend to be irritant.
As well as irritant reactions, there are also allergic and phototoxic ones, and of the three, allergic reactions are the most common. If you have an irritant reaction, it makes sense to apply something to the skin to dilute any remaining essential oil. However, allergic reactions are quite different. If you have one, well you have just become allergic to something, meaning you may never be able to use it again without having another, similar reaction. You can find out more about allergic reactions to essential oils, and how to avoid them, here.
Because essential oils consist of small, volatile compounds that easily interact with TRP channels, they can – potentially – irritate skin, gut and airways. Because they can also penetrate the skin, essential oils do represent particular risks. However, these same properties also convey benefits.
Menthol, for example, activates TRPM8, and this channel registers cold temperature (Liu et al 2013). This means that Peppermint oil, which contains about 40% menthol, feels cold on the skin. The skin’s temperature does not change, but our body reacts as if it was sensing cold – blood rushes to the area in order to warm it. So although Peppermint oil and menthol are often thought of as cooling, they are also warming, and in a more real sense.
Another action of menthol, via TRP channels, is analgesia (Liu et al 2013). The combination of analgesia and other properties makes Peppermint oil especially useful for muscular pain, neuropathic pain and most types of itch. For neuropathic pain, 0.5-1% menthol is effective meaning that 1-2% Peppermint oil would also work well (Colvin et al 2008, Storey et al 2010).
The devil is in the dilution
Another major function of our skin is to keep harmful substances and microbes outside of our body, and there are several ways in which our body protects us. First, there is the skin barrier consisting of many layers of skin cells, arranged in a way that makes penetration extremely difficult. If an “intruder” manages to make it through the barrier, the immune system kicks in, pumping in more blood and launching a defensive cascade called the inflammatory response. This may manifest as redness, bumps, itching, or painful sensations.

Essential oils can calm irritation or inflammation, but it’s hugely important to understand the importance of dilution. Some of the same essential oils can irritate or calm, depending on dilution. For example, citronellol (Rose otto, Geranium) and geraniol (Palmarosa, Rose otto, Geranium) are both TRPV1 activators (Denda et al 2010), but in dilution they – both constituents and essential oils – are among our most potent anti-inflammatory agents (Abe et al 2003, Abe et al 2004, Katsukawa et al 2011, Kobayashi et al 2016, Maruyama et al 2005, Ye et al 2019).
In fact, TRPV1 modulators can be expected to be therapeutic for itch, skin barrier disruption, heat pain, and photoaging (Lee et al 2012, Tang et al 2022). TRPA1 is another relevant channel. In an in vitro study, linalool activated TRPA1 at 100 micromoles, and blocked TRPA1 at 500 micromoles (Batista et al 2011, Reira et al 2009). Menthol and camphor are also TRPA1 modulators – the effect depends on the concentration.
This is starting to sound complicated! How do we know what dilutions to use?
How much to dilute and why?
Assuming you always want to minimize risk while maximizing the potential benefits, how do you dilute, and why? As I mentioned earlier, we will be talking percentages, not drops. Percentages can be converted to any measurement, any scale, and if you’re not sure about measuring, I can recommend one of our single classes: Essential Calculation with Hana Tisserand (it is our most popular single class.) Establishing approximate dilution ranges is not difficult, and I have been promoting charts like this for some time: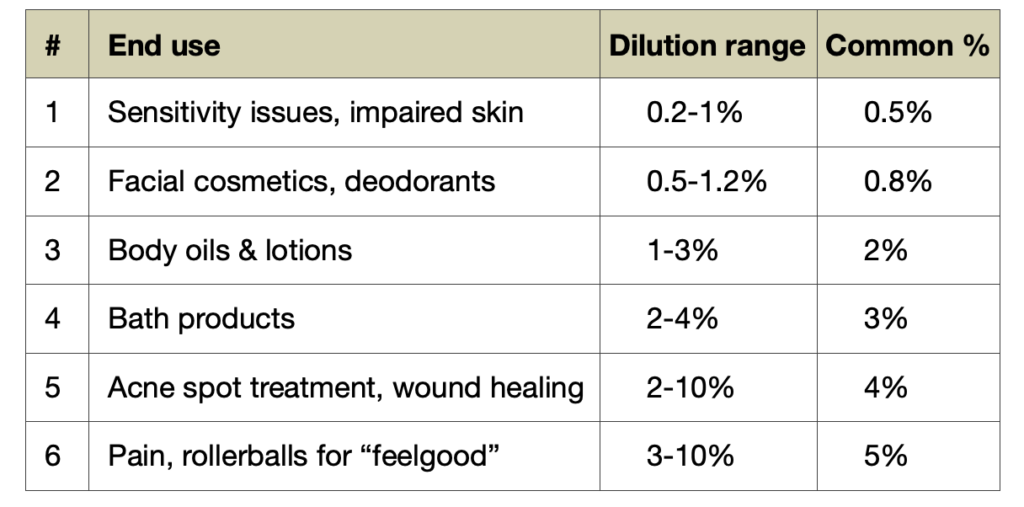 So let’s dive into it. There are six dilution ranges, according to the intended use. Think of these not as rules, but as useful guidelines. There may be exceptions in particular cases, but these percentages will give you a good idea of sensible dilutions – ones that are both effective and safe. As I mentioned earlier, the greater the concentration of essential oil, the greater the risk of an adverse skin reaction.However, the same does not apply to therapeutics. Increasing dose or concentration up to a certain level does also increase therapeutic potency, but at a certain point this reaches a plateau, and going from, say 5% to 10% does not add any extra benefit. In other words, increasing concentration always increases risk, but may not increase benefit.
So let’s dive into it. There are six dilution ranges, according to the intended use. Think of these not as rules, but as useful guidelines. There may be exceptions in particular cases, but these percentages will give you a good idea of sensible dilutions – ones that are both effective and safe. As I mentioned earlier, the greater the concentration of essential oil, the greater the risk of an adverse skin reaction.However, the same does not apply to therapeutics. Increasing dose or concentration up to a certain level does also increase therapeutic potency, but at a certain point this reaches a plateau, and going from, say 5% to 10% does not add any extra benefit. In other words, increasing concentration always increases risk, but may not increase benefit.
Depending on the specific situation, you may need to adjust (see this post about blending for cosmetic products). A very useful rule of thumb is to start low and increase the concentration only if needed.
These ranges have been developed based on research in both safety and efficacy. Here’s a more detailed rationale for each:
Range 1 – Sensitivity issues, impaired skin 0.2-1%
This is for someone whose skin is already reaction-prone, or has impaired barrier function. We need to be extra careful and introduce essential oils in very low concentrations to avoid exacerbating the situation. Close monitoring is encouraged in these cases.
Range 2 – Facial cosmetics and deodorants 0.5-1.2%
For many cosmetic effects (dry skin, aging skin etc) this range is generally what we want (Altaei 2012, Auffray 2007, Reuter et al 2008). This second lowest range is intended for application to the face and other sensitive areas, such as underarms.
Range 3 – Body oils and lotions 1-3%
This dilution range has been in use for more than 50 years by aromatherapists for body massage with essential oils, and it also corresponds with the range of fragrance used in commercial personal care products.
Range 4 – Bath products 2-4%
This category includes wash-off products (soap, body wash etc) and any products to be used in the bath or shower. Wash-off products don’t linger on our skin, while bathing assumes the essential oils will be evenly dispersed in the bathwater, and therefore diluted even further. We do want to enjoy an aroma that is easily perceptible, and so the range is slightly higher.
Range 5 – Acne spot treatment, wound healing 2-10%
This range is based on what research shows are effective concentrations. From clinical trials we know that 5% is an effective dilution for acne, as well as for itch (Elsaie et al 2016, Enshaieh et al 2007). Here we’re entering the therapeutic application zone and we need to make sure we have enough punch in our product to deal with the issue, while still avoiding adverse reactions. This also assumes short-term, targeted application. If you’re not seeing any results at 10% essential oil, you may need to reconsider the treatment regimen.
Range 6 – Pain and “feel good” rollerballs 3-10%
For menstrual pain, clinical studies use concentrations of 3-5% (Sut & Kahyaoglu-Sut 2017). For musculoskeletal pain, up to 10% might be needed, but 1.5-5.0% is often effective (Bako et al 2023). Most painful conditions that are addressed with essential oils are not at the level of skin, but rather muscle and connective tissue, and therefore we may need a higher concentration to get the desired effect. Adjust up or down based on how acute the condition is. For rollerballs, the dilution assumes that they are used on small area of skin. If you have sensitive skin, you may consider either applying the oils to clothing, or using a jewelry diffuser such as a pendant.
Finally, this Table applies to all essential oils, except those that carry specific restrictions. You can find the IFRA restrictions on their website, but it’s not the easiest to navigate, and most of them only apply to constituents. You will also find most of them in Essential Oil Safety, a book I co-authored in 2014, and here the constituent maxes are applied to essential oils. You can also check the Tables of the most irritant and allergenic essential oils, along with their maximums, in this article.
Dilution can make or break your skin
I wanted to give you an example of a product that may have all the right ingredients, but with, in my opinion, an inappropriate dilution which renders the potential benefits nonexistent. The product is made by DoTerra, and it’s their Immortelle Anti-Aging Blend. It’s for direct application to the face, and consists of undiluted essential oils of Frankincense, Sandalwood, Lavender, Everlasting, Rose and Myrrh. The directions and intended effects are:
- Apply a thin layer to the face, neck, and décolletage, then repeat application to targeted areas of concern. Follow with the doTERRA moisturizer of your choice.
- Include in a morning and night facial routine.
- Helps to reduce the appearance of fine lines and wrinkles
- Helps reduce contributing factors to the appearance of aging skin
- Helps sustain smoother, more radiant, and youthful-looking skin
In my opinion, this would all be totally fine if the product contained about 1% of essential oil instead of 100% as many of the oils in the product do have relevant properties. The following guideline is also included on the product page: “Dilute with a carrier oil to minimize any skin sensitivity”. This is better than not having anything, but it feels like an inadequate after-thought. If you did have an allergic reaction to the product this is not something that you can just make go away by dilution after the fact.

Here’s an account from one person who had a bad reaction to Immortelle Anti-Aging Blend:
“I used it initially in a blend, on my face directly. As my husband said: “looks like some bad Botox.” Everywhere I applied was puffy, red and itchy…yet it didn’t actually show up for about 24 hours. I then noticed their blend was not diluted (probably should have looked for that first) and applied FCO to it for a week. It subsided, although continued to itch for some time and peeled slightly upon healing.”
The full report is HERE.
Definitely not the experience you hope to have after spending a substantial amount of money to get radiant skin. The user quickly established that it was the Frankincense oil in the blend that was causing their reaction. This was extremely useful for them to know, so they could avoid it in future. Also note that applying fractionated coconut oil for a several days did not prevent the itch.
Here, here, here and here are other reports of reactions to Everlasting/Immortelle/Helichrysum oil (that’s one oil with several names) or one of the Frankincense oils when applied undiluted. And there are many more reactions to other undiluted oils in our database.
Another issue with undiluted essential oils is that they are drying on the skin – just like alcohol – because of the evaporation. Even dilutions can be drying. In one report, Peppermint and Tea Tree oils were not drying at 1%, but at 5% both had a slightly drying effect. The oils were applied solubilized in water, using an emulsifier (Nielsen 2006).
If you look at commercial facial and body care products, fragrance concentrations are very much in line with what I have indicated in the above chart. Facial products very often have about 0.5% fragrance. It’s true that these fragrances are there only to make the product smell good, and in most cases not to be therapeutic. Still, going from 0.5% to 100% makes no sense!
The good news is that you can always dilute, so if you have this product, please make sure to mix it with an suitable medium of your choice.
Legislation
As we established, some essential oils do cause adverse reactions. In every case this is concentration-dependent (Johansen et al 1996). Because essential oils can cause adverse reactions they are very often cautioned against by dermatologists. For example, in this article, Los Angeles-based dermatologist Divya Shokeen says: “Some essential oils may be more irritating than others, so it’s important to do your research and consult with a dermatologist if you have any concerns. The only undisputed truth: You should never apply undiluted essential oils to your skin.” And because some essential oils can cause adverse reactions, their use has been regulated by various consumer protection bodies.
In an attempt to address the issue of adverse reactions, the EU passed legislation requiring cosmetics to be labelled if a leave-on product contains more than 0.001% of any of the following essential oil constituents:
Anise alcohol
Benzyl alcohol
Benzyl cinnamate
Benzyl salicylate
Cinnamaldehyde
Cinnamyl alcohol
Citral 
Citronellol
Coumarin
Eugenol
Farnesol
Geraniol
Limonene
Linalool
And these two absolutes:
Treemoss absolute
Oakmoss absolute
This only requires a labelling declaration if any essential oils result in the level of 0.001% being exceeded. (This 0.001% is, but the way, an arbitrary restriction that has no scientific basis.) However, many retail establishments in Europe will not sell products that require allergens to be listed, because they do not want to be associated with products that may be perceived as unsafe.
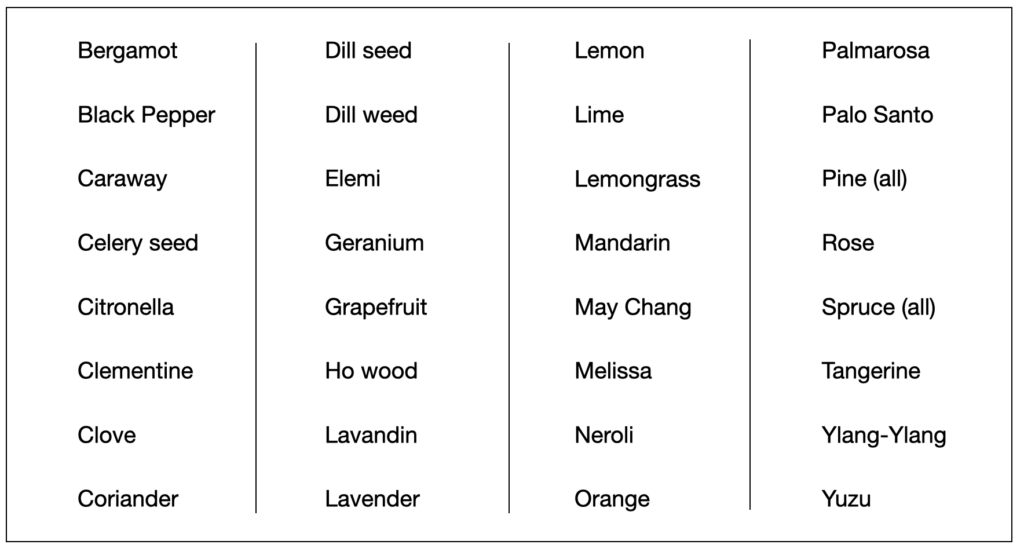
Table of essential oils containing at least one of the restricted constituents.
These restrictions, if implemented as maximums, would virtually eliminate many essential oils from being used in fragrances or cosmetics (limonene is found in dozens of essential oils). The list would include all the oils shown in the Table, and more.
The legislation exists because it is an attempt to reduce cases of adverse reactions to fragrant products. I would say that it’s well-meaning, but poorly implemented, since some of these so-called allergens carry minimal risk. For example, out of 1,508 people who were patch tested, none reacted to limonene or geraniol, and only 0.1% (1 in 1,000) reacted to linalool, citronellol, benzyl cinnamate and anise alcohol. In contrast, 1.35% (1 in 77) reacted to cinnamaldehyde – 13 times as many (Heisterberg et al 2011).
Another body regulating essential oil dilutions and giving safe ranges is IFRA (International Fragrance Association). One notable difference between the EU legislation and IFRA regulations, is that IFRA uses evidence-based maximums. For example, the EU max for limonene is 0.001%, and the IFRA max is 1.25% (to avoid phototoxicity). For geraniol, the EU has 0.001% while IFRA has 4.7%. Essential Oil Safety, 2e (a textbook I co-authored), talks about EU and IFRA regulations and explains where those may be overcautious. However, if you want to sell your product to the general public in Europe, you do need to comply, even if the guidelines sometimes make no sense.
What do we do then?
So we have one group (the EU) suggesting that some essential oils would only be safe on the skin at about 0.01% (once you extrapolate from the constituents) and yet, at the same time, we have folks selling products consisting of 100% essential oil. Who is right here?
The answer is very much in the middle. I would suggest that neither of these approaches is correct, and I regard them both as extremes. Extreme foolishness, or extreme paranoia. Is Lemon oil safe at 100% or only 0.01%? The IFRA safe limit for Lemon oil (to avoid phototoxicity) is 2%, which is almost exactly in between 0.01% and 100%. This is the safe maximum, not a recommended amount, which might be less, and for that we would consult the chart.
Like any active ingredient, there are risks associated with essential oils, and using them undiluted on the skin is neither sensible nor necessary. For an in-depth journey into safety and skin, you could check out these Tisserand Institute certification courses:
https://tisserandinstitute.org/essential-oil-safety-master-class/
https://tisserandinstitute.org/skin-course/
References
Abe, S., Maruyama, N., Hayama, K., Inouye, S., Oshima, H., & Yamaguchi, H. (2004). Suppression of neutrophil recruitment in mice by geranium essential oil. Mediators of Inflammation, 13(1), 21–24. https://doi.org/10.1080/09629350410001664798
Abe, S., Maruyama, N., Hayama, K., Ishibashi, H., Inoue, S., Oshima, H., & Yamaguchi, H. (2003). Suppression of tumor necrosis factor-alpha-induced neutrophil adherence responses by essential oils. Mediators of Inflammation, 12(6), 323–328. https://doi.org/10.1080/09629350310001633342
Altaei, D. (2012). Topical lavender oil for the treatment of recurrent aphthous ulceration. American Journal of Dentistry, 25(1), 39–43.
Auffray, B. (2007). Protection against singlet oxygen, the main actor of sebum squalene peroxidation during sun exposure, using Commiphora myrrha essential oil. International Journal of Cosmetic Science, 29(1), 23–29. https://doi.org/10.1111/j.1467-2494.2007.00360.x
Bakó, E., Fehérvári, P., Garami, A., Dembrovszky, F., Gunther, E. E., Hegyi, P., … Böszörményi, A. (2023). Efficacy of topical essential oils in musculoskeletal disorders: systematic review and meta-analysis of randomized controlled trials. Pharmaceuticals, 16(2). https://doi.org/10.3390/ph16020144
Batista, P., Harris, E., Werner, M., Santos, A., & Story, G. (2011). Inhibition of TRPA1 and NMDA channels contributes to anti-nociception induced by (-)-linalool. The Journal of Pain, 12(4). https://doi.org/10.1016/j.jpain.2011.02.122
Colvin, L. A., Johnson, P. R. E., Mitchell, R., Fleetwood-Walker, S. M., & Fallon, M. (2008). From bench to bedside: A case of rapid reversal of Bortezomib-induced neuropathic pain by the TRPM8 activator, menthol. Journal of Clinical Oncology, 26(27), 4519–4520. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/18802169
Denda, M., Tsutsumi, M., & Goto, M. (2010). Topical application of TRPA1 agonists and brief cold exposure accelerate skin permeability barrier recovery. Journal of Investigative Dermatology, 130, 1942–1945. https://doi.org/10.1038/jid.2010.32
Elsaie, M. L., Almohsen, A. M., Ibrahim, I. M., & Mohey-Eddin, M. H. (2017). Effectiveness of topical peppermint oil on symptomatic treatment of chronic pruritus. Clinical, Cosmetic and Investigational Dermatology, 9, 333–338. https://doi.org/10.1111/jocd.12342
Enshaieh, S., Jooya, A., Siadat, A. H., & Iraji, F. (2007). The efficacy of 5% topical tea tree oil gel in mild to moderate acne vulgaris: a randomised, double-blind placebo-controlled study. Indian Journal of Dermatology, Venereology, and Leprology, 73(1), 22–26.
Heisterberg, M. V, Menné, T., & Johansen, J. D. (2011). Contact allergy to the 26 specific fragrance ingredients to be declared on cosmetic products in accordance with the EU cosmetics directive. Contact Dermatitis, 65(5), 266–275. https://doi.org/10.1111/j.1600-0536.2011.01962.x
Johansen, J.D., Andersen, K.E., Rastogi, S.C., Menne, T. (1996). Threshold responses in cinnamic-aldehyde-sensitive subjects: results and methodological aspects. Contact Dermatitis, 34, 165–171.
Katsukawa, M., Nakata, R., Koeji, S., Hori, K., Takahashi, S., & Inoue, H. (2011). Citronellol and geraniol, components of rose oil, activate peroxisome proliferator-activated receptor α and γ and suppress cyclooxygenase-2 expression. Bioscience, Biotechnology and Biochemistry, 75(5), 1010–1012. https://doi.org/10.1271/bbb.110039
Kobayashi, Y., Sato, H., Yorita, M., Nakayama, H., Miyazato, H., Sugimoto, K., & Jippo, T. (2016). Inhibitory effects of geranium essential oil and its major component, citronellol, on degranulation and cytokine production by mast cells. Bioscience, Biotechnology and Biochemistry, 80(6), 1172–1178. https://doi.org/10.1080/09168451.2016.1148573
Lee, Y. M., Kang, S. M., & Chung, J. H. (2012). The role of TRPV1 channel in aged human skin. Journal of Dermatological Science, 65(2), 81–85. https://doi.org/10.1016/j.jdermsci.2011.11.003
Liu, B., Fan, L., Balakrishna, S., Sui, A., Morris, J. B., & Jordt, S. E. (2013). TRPM8 is the principal mediator of menthol-induced analgesia of acute and inflammatory pain. Pain, 154(10), 2169–2177. https://doi.org/10.1016/j.pain.2013.06.043
Maruyama, N., Sekimoto, Y., Ishibashi, H., Inouye, S., Oshima, H., Yamaguchi, H., & Abe, S. (2005). Suppression of neutrophil accumulation in mice by cutaneous application of geranium essential oil. Journal of Inflammation, 2(1). https://doi.org/10.1186/1476-9255-2-1
Nielsen, J. B. (2006). Natural oils affect the human skin integrity and the percutaneous penetration of benzoic acid dose-dependently. Basic and Clinical Pharmacology and Toxicology, 98(6), 575–581. https://doi.org/10.1111/j.1742-7843.2006.pto_388.x
Reuter, J., Huyke, C., Casetti, F., Theek, C., Frank, U., Augustin, M., & Schempp, C. (2008). Anti-inflammatory potential of a lipolotion containing coriander oil in the ultraviolet erythema test. Journal Der Deutschen Dermatologischen Gesellschaft, 6(10), 847–851. https://doi.org/10.1111/j.1610-0387.2008.06704.x
Riera, C. E., Menozzi-Smarrito, C., Affolter, M., Michlig, S., Munari, C., Robert, F., … Le Coutre, J. (2009). Compounds from Sichuan and Melegueta peppers activate, covalently and non-covalently, TRPA1 and TRPV1 channels. British Journal of Pharmacology, 157(8), 1398–1409. https://doi.org/10.1111/j.1476-5381.2009.00307.x
Storey, D. J., Colvin, L. A., Mackean, M. J., Mitchell, R., Fleetwood-Walker, S. M., & Fallon, M. T. (2010). Reversal of dose-limiting carboplatin-induced peripheral neuropathy with TRPM8 activator, menthol, enables further effective chemotherapy delivery. Journal of Pain and Symptom Management, 39(6), 2–4. https://doi.org/10.1016/j.jpainsymman.2010.02.004
Sut, N., & Kahyaoglu-Sut, H. (2017). Effect of aromatherapy massage on pain in primary dysmenorrhea: A meta-analysis. Complementary Therapies in Clinical Practice, 27, 5–10. https://doi.org/10.1016/j.ctcp.2017.01.001
Tang, L., Gao, J., Cao, X., Chen, L., Wang, H., & Ding, H. (2022). Chemical composition and antifungal activity of essential oil of Salvia sclarea L. from Bulgaria against clinical isolates of Candida species. Experimental Dermatology, 31(3).
Tisserand, R., Young, R. (2014). Essential oil safety: a guide for health care professionals. Churchill Livingstone, Edinburgh.
Ye, C. J., Li, S. A., Zhang, Y., & Lee, W. H. (2019). Geraniol targets KV1.3 ion channel and exhibits anti-inflammatory activity in vitro and in vivo. Fitoterapia, 139. https://doi.org/10.1016/j.fitote.2019.104394

0 Comments